
[ad_1]
Dr. Benjamin Co, an expert in infectious diseases and clinical pharmacology, has been fortunately breaking down the coronavirus numbers on your personal blog since the outbreak started. The insight it provides is informative and comforting for those who want a clear picture of how we deal with the virus. Dr. Co will share daily updates and analysis of the numbers reported by the Department of Health with ANCX.
–
See link DOH.gov.ph or updated data or COVID19.gov.ph. (The latter is not a secure site). The new site for the Department of Health is easy to use, provides more information where you see a COVID19 tracker. Readers can refer to their official site where Data Drop can be found for raw data.
A useful site is COVID19stats, where you can see most DoH data in graphical format.
Transparency and the exchange of vital information is important as part of good governance. After all, these data are used as models and prediction scales to serve as platforms for planning in the business sector. Uncertainties are quantified and qualified to make a country more prepared for a pandemic of this magnitude.
You may also like:
If there is no reliable and timely information provided by the health department, one cannot help but wonder where the data is being obtained from and the quality of the data being shared to the public as part of public information. Selective announcement of data is never recommended because it creates disinformation when news is delivered about the actual outbreak situation in the country. Is it a deliberate concealment of data, or is it a reflection of the competition (or lack thereof) of the respective agencies?
It cannot be overemphasized that the only way we will beat this pandemic is if we do more aggressive and intensive contact tracing, testing and isolation, and quarantine those who test positive for the virus in the community.
The DoH reported 264 new cases, 107 new recoveries and 25 new deaths. Compared to globally confirmed cases, the Philippines contributes 0.27 percent of cases and 0.26 percent of COVID-19 deaths worldwide.
Two things to remember with daily data analysis:
(1) These three parameters (new confirmed cases, new recoveries, new deaths) are not real-time data. The data provided by the Department of Health is the date of the public announcement. It is actually very, very late.
(2) Depending on where the tests are performed, the RT-PCR test results take an average of one to two days to process. Unless there are delays, all tests performed should ideally be released for at least 48 hours (the sooner the better). However, the results of tests published at government facilities vary from three to 14 days, probably due to the large number of tests that are performed compared to private hospitals where fewer tests are performed.
New announced cases, recoveries and deaths are the count of reported cases for the day.

Comparison of new daily cases, deaths and daily recoveries. There are now 2,857 cases closed.
Case fatality increased 6.64 percent (from 6.73 percent of the world average vs. 2.44 percent of the ASEAN average) and the recovery rate increased to 19.4 percent (from 37 percent). percent of the world average vs. 30 percent of the ASEAN average) for the day.
The Philippines case fatality rate will soon reach the world average case fatality rate. (Note that a few weeks ago the world’s CFR was at 7.75 percent. With more global testing and tracking, there are now fewer deaths and more reported asymptomatic cases. Even within the ASEAN region, the average death rate is lower compared to ours and the average recovery rate is higher than in the Philippines). Which means only one of two things: We are not doing enough testing and tracking and / or our health system is really bad. No matter how the authorities try to provide excuses for the data, it keeps going back to the quality of the data available.
The doubling time allows us to know the number of days it takes to double confirmed cases (or death rates) and can be determined linearly or exponentially. A logarithmic scale is the ideal graph to use. The following figure shows that the doubling time in mortality rates is around 8.3 days. The case growth rate is now 2.29 percent (based on the 7-day average).
DOH Reporting
More than half (399) are posthumous results. This is the number of people who died before being declared positive for SARS-CoV-2.
A follower who was also tracking the data with me noticed an even bigger problem with data entry.
Of the 114 deaths announced last week (May 6-12), the actual date of deaths is 21 days on average! Many are over 30, over 40 and even up to 52 days ago. (Thirty-seven of the 114 do not have a “Date of Death” entry.)
While the average latency was nine days last month, it is now getting much worse.

Report of deaths in the data fall of the Department of Health.
The figure above shows a snapshot of so many errors entered. For example, the first date for C129601 shows the date you tested positive (report confirmed) on April 8, 2020. The next column shows the date of death. Is this really March 4, 2020 or was it entered incorrectly? Because if he died on March 4, 2020, the last column shows that he was publicly reported on April 20, 2020! The delay from death to confirmation of the complaint is staggering! For patient C130591, she tested positive on the lab on March 7, 2020. But she passed away on 12/3/2020 (would that mean the entry was incorrect and should probably have been on 12/3/2020?). And it was reported the same day assuming it was an incorrect entry.
A snapshot with two cases as an example. If you go through all the fields in the data drop, I’d say they just delete it entirely and probably create a secret file of our own instead of making us try to make sense of your data entry and reporting system.
I can’t even understand how someone there can make heads of these reports they produce and use them as a basis for the President or the IATF to make recommendations for blockades. The way reports come out, it’s like Russian roulette. We don’t know when the lone bullet in the loaded gun will be fatal to us.
The need for a more timely reporting of all input data cannot be overemphasized. This includes all tests, deaths, and recoveries. Latent reports are useless because they do not reflect the true state of the pandemic in the country and whether policies like ECQ or MCQ or GCQ really work or not. What is happening is that we are simply “guessing” that with the blockade mitigation strategy, we have decreased the number of cases in the country.
This theory is partially flawed because when the ECQ was stated, the measures on how to deal with it must have been planned and implemented immediately. In short, the government should have already planned B. While it is working to run more tests and arguably the government had announced this morning that they were not doing enough contact tracking, it would now make efforts on this, we are actually behind schedule. 60 days plan. It makes you wonder when a real date would be when all data would be in real time. Because as long as latent data is the basis for policy making, these poor data quality based policies will always be flawed.
New cases per day
Of the 268 new cases announced today, all had been tagged with their residence information. One hundred sixty-five (61 percent) were from the NCR, 58 (22 percent) from Region VII, and 45 (17 percent) from other areas. Region-level data is accurate, but cases by city are reported only for those that could be verified. There were still a handful of validations as of this report.
In the NCR, the breakdown is as follows: Quezon City (27), Manila (5), Parañaque (12), Makati, Muntinlupa and Malabon (2 each), Mandaluyong, Las Piñas, Valenzuela and Pateros (1 each) , Marikina (3), Pasay (8), Taguig (11), Pasig (6), Caloocan and Marikina (3 each). There were still 80 cases to validate.
Region VII reported 46 cases in Cebu city, 5 in Cebu province, 1 in Mandaue, and 6 in Lapu Lapu city.
Other reporting areas include: Mindoro Oriental (1), Ciudad de Zamboanga (17), Baguio (1), Ifugao (1), Rizal (4), Laguna (5), Cavite (2), Batangas (4), Lucena (2), Cagayan de Oro (1) and Cotabato (1). The rest are for validation.
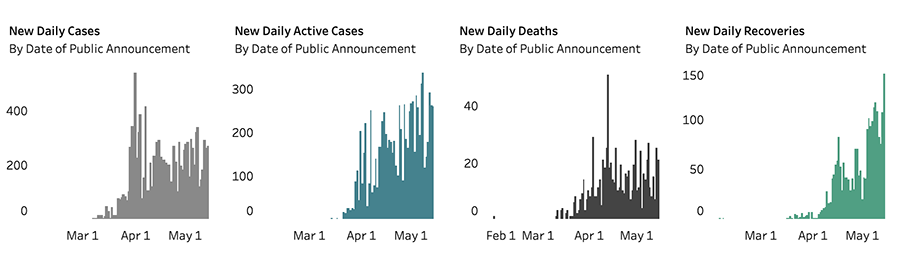
New daily cases, deaths and recoveries.
The DoH website update shows the bar graph (Figure 4) for daily cases, active cases, daily deaths, and daily recoveries. Although there has been a decrease in the last 3 days in new daily cases, today there is a stable number of new cases. The only predictable good news is the continued increase in daily recoveries. However, deaths remain the main indicator of how the country can cope with the outbreak, considering that the Philippines is a country with a very young median age of 27.8 years.
Tests
There were no reports for the tests since May 10. Today, they published the number of tests performed, adding that 15,373 tests were conducted over a two-day period.
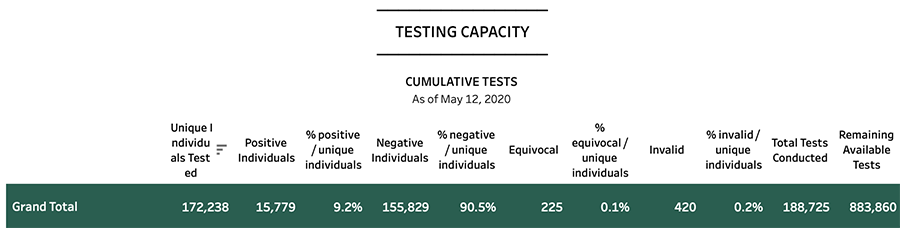
Test capacity in terms of number of tests performed
Of the total of 188,725 tests carried out so far on 172,238 people, at least 9.2 percent (15,799) yielded positive results, with 90.5 percent negative. The rest were equivocal or invalid and were not included as part of the count. Remember, positive results are not equal to the number of new confirmed cases because positive cases will need to be retested until they return to two negative results.
No matter how many tests we do per day, it’s not just the volume that matters. It is the timely publication of the test results. If the Philippines brags that it can do 30,000 tests a day, let’s hope that those 30,000 are released in a timely manner. The essence of testing is to track contact and treat or isolate patients who are positive.
To contact the Department of Health, the COVID hotline is (02) 894-COVID loc 1555.
Global statistics
Update starting at 9 p.m. from May 13, 2020 (Wednesday)
TOTAL CONFIRMED CASES: 4,355,456
TOTAL DEATHS: 293,090 (fatality rate: 6.73 percent)
TOTAL RECOVERED: 1,610,421 (case recovery rate: 37 percent)
Total cases worldwide
Please note that each reference has its own cutoff time to report. For global data, WorldOMeters is used as a reference.
Total confirmed cases have passed the 4M mark as previously predicted. The average trend in the past week has averaged 100,000 new cases confirmed daily with more tests conducted worldwide. At the current growth rate, at least 1 million new confirmed cases can be registered every 10 days. This means that there is a high probability that the 5M mark will be reached on or before May 19, 2020.
The total number of recoveries has passed the 1.5M mark with recoveries significantly greater than deaths.
The United States of America continues to lead the world in the total number of confirmed cases at 1,408,636 with a case fatality rate (CFR) of 5.92 percent with 83,425 total deaths recorded. The recovery rate for the USA USA It increased 21.1 percent. Among the states, New York leads nearly 348,655 total confirmed cases and 27,175 total deaths with a stable CFR at 7.8 percent. The growth rate of new cases and deaths has slowed significantly in New York. Until yesterday, almost 10 million tests have been carried out (30,017 / M population).
While the United States may have the highest number of cases and the number of deaths in the world, Belgium (16.29 percent), Yemen (15.69 percent), and France (14.9 percent) have the highest mortality rates. 9 countries with more than> 50 cases AND zero (0) deaths reported by COVID-19 are: Vietnam, Cambodia, Uganda, South Sudan, Rwanda, Madagascar, Mozambique, Central African Republic and Nepal for more than two weeks.
Iceland now has the highest case recovery rate with 98.45 percent recovered (1,773 recoveries, 10 deaths in 1801 confirmed cases in total). Cambodia’s recovery rate remains at 98.36 percent (120 of 122 cases) no deaths reported since his first COVID-19 case. Cambodia has not had a new case since April 13, 2020.
The average case-fatality rate worldwide remains 6.73 percent. Based on current data for the past 2-3 months, about 80-90 percent of patients are asymptomatic or recover remarkably. Depending on the country’s health system and the risk age group (major or minor populations), the mortality rate is between 5 and 15 percent on average. Recoveries far outweigh deaths with a ratio of approximately 5.5: 1.
