
[ad_1]
How decisive was the Dpcm on November 6 during this second wave of Covid19? The Conte government had divided Italy into three risk zones in the hope of improving the situation, but based on analyzes carried out by Open together with physicist Enrico D’Urso it is less effective than the blockade implemented at the beginning of the pandemic.
A gentle route was chosen with respect to the lockdown, for economic and social reasons, but without decisively slowing down the spread of the virus and consequently infections. During the approval of the Dpcm on November 6, there was already a decrease in increases in intensive care, and then a slow decline began that did not depend on government measures but on the number of deaths. What is clear is that a mitigation of the spread of the virus has been achieved, not a sharp decline, in fact the graphs show that hospitals empty more slowly, precisely because new infections continue to appear and consequently new patients.
This article follows the previous one on November 14, where we analyze the differences between the first and second waves, taking into account the number of hospitalizations, intensive care and deaths in relation to the maximum capacity of hospitals to treat serious cases (SSN) . , values that help us better understand how the new coronavirus spreads in Italy.
The situation before the Dpcm
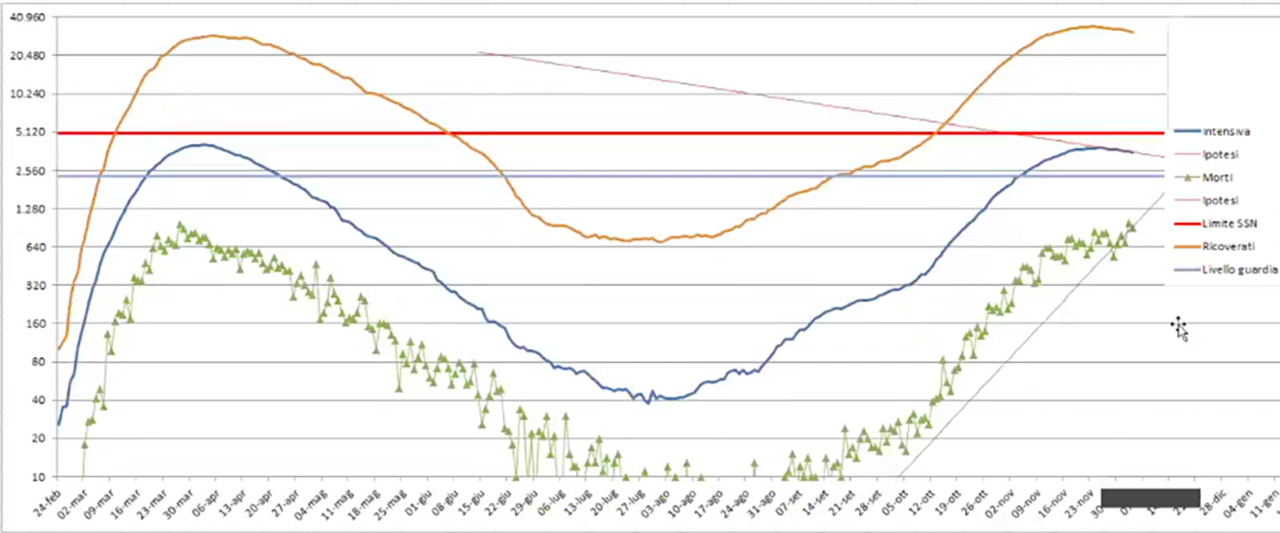
The curve of hospitalized patients with severe forms of Covid-19 was approaching the NHS limit, set at 5,000 places in intensive care with a maximum of 7,000 in relation to the total number of places, taking into account that the health emergency could also have absorbed the beds. intended for other departments.
By overlaying the curves of the first and second waves, matching their start dates on the graphs, the proportions between hospitalized patients, ICU and deaths were lower than in the first peak. These data made us reflect on how little prepared we were for the appearance of the virus.
In the first part of the pandemic we have many deaths from intensive care. We did not know what therapeutic protocols to adopt and we had a large number of sick elderly people, while at the beginning of the second peak there were few elderly people and we knew what medical measures to take.
The capacity limit of the hospitals was an avoidable risk, in addition to reaching a peak and then initiating a decline, not only for the healed, but also for the dead. A constant is maintained, namely, the presence in the population of higher risk subjects that are reflected in the graphs observed in the previous article.
Let’s now see what happened during the last Dpcm, pending the entry into force of the most recent one from December 21 to January 6, after which we will look at the charts again.
Intensive care: Dpcm had little influence
Compared to the lockdown, we have regions with lighter measurements (orange and yellow areas), compared to others with greater restrictions (red areas). As emerged in the documents relating to the act of Scientific Technical Committee – notice thanks to a request for Einaudi Foundation – This division into three types of regions had been deliberately ignored by the Giuseppe Conte administration, which led to the closure and provoked various criticisms.
As we can see in the first graph, the ICU admissions curve (blue line) had already been falling for about a month, so it was physiological for a hump to form and then decrease. In other words, the trend was linear and no longer exponential, as would be expected from a virus of this type, if it were allowed to circulate freely. The problem was not letting it continue beyond the capacity limit, anticipating the decline as much as possible, because statistically we will have in proportion not only recovered patients, but also victims.
Hospitals empty more slowly
The second peak comes on November 25, with 3,848 intensive care units occupied (with an estimated limit of 5,000), in addition to starting to decline. How fast compared to the first peak?
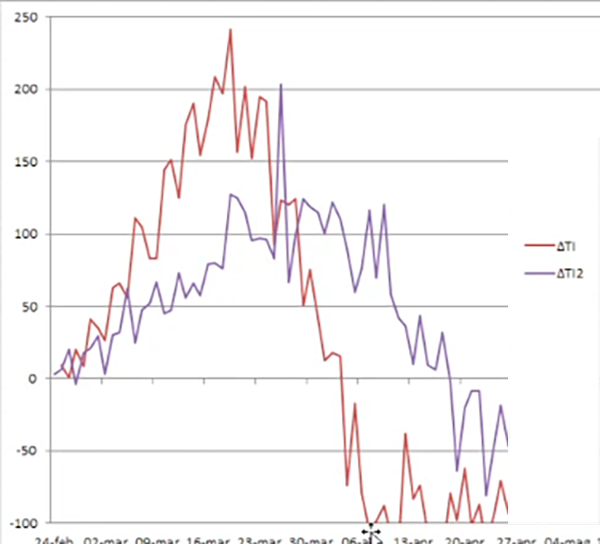
In the second graph we see a comparison of the increases (above zero) and decreases (below zero), between the first and second waves (red and blue lines respectively). The lockdown is associated with a steeper drop in ICU admissions than seen during the Prime Minister’s Decree of November 6.
To get an idea of what might have happened, let’s go over a few concepts, which you can learn more about in our previous articles. The reproduction rate of SARS-CoV-2 (Ro = 2) is such that it has an exponential spread of Covid-19 and is an intrinsic property of the pathogen. With the advent of containment measures, such as social distancing, the transmission index (Rt) is considered, which does not depend only on the virus, but above all on the presence of obstacles to its spread.
Consequently, having a low Rt does not necessarily indicate a narrow escape, but only that there is some barrier to the spread of the epidemic, so the development of suitable vaccines is always the best possible measure to integrate with others.
Because having fewer busy ICUs is not always good news
It is also true that hospitals and medical personnel must be kept at their best, so it is necessary not to penalize the country’s economy beyond a certain threshold. Observing this phase of decline we have seen that intensive care empties, although more slowly: what does it mean?
The third graph shows the relationship between intensive care and hospitalization (green line), between deaths and intensive care (blue line), and the average weekly trend of the relationship (red line).
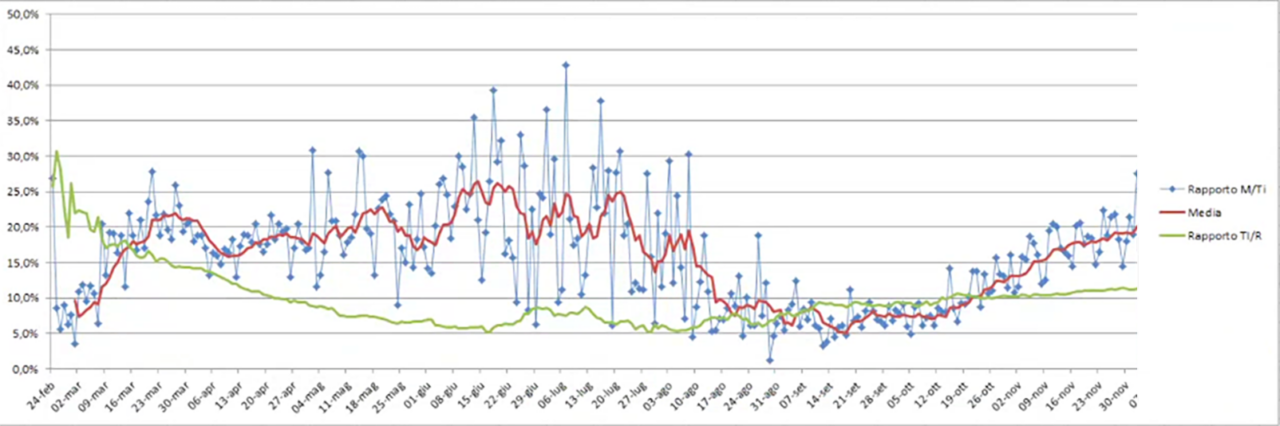
We see that there is little to be happy about, because deaths are on the rise: it is these that have a particular impact on declining jobs. As of December 4, the death / intensive care ratio was approximately 20%. We note in particular that during the summer mainly young people became ill, now the average age of seriously ill patients is increasing.
Good but not great
In the last graph we see an overlap in ICU admissions between the first wave (blue line) and the second wave (red line).
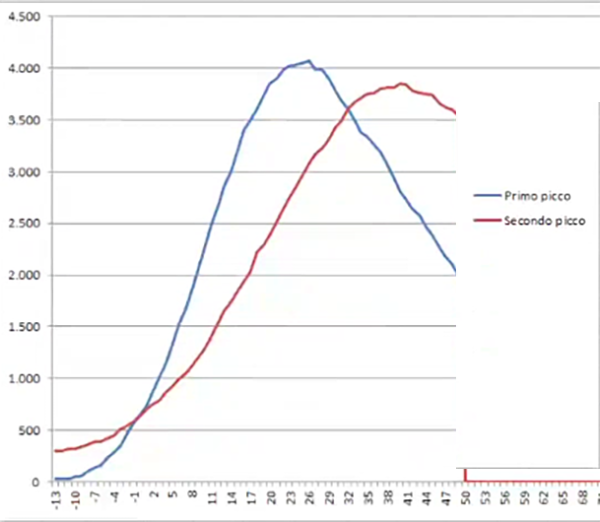
In the first wave the descent was faster, but this was due to the fact that there were many more deaths. In the second wave, more people get sick, but over a longer period of time. Compared to the charts, the latest DPCM seems to mitigate the curve without clearly improving the situation.
We have preferred less rigid measures in the long term to more rigid ones in the short term, to satisfy understandable economic needs. Taking this into account, it may not be a great sacrifice to face the new measures planned during the holidays, since the objective is to experience many more in the coming years, possibly together with the members who tend to bring families closer together on these occasions, generally the older ones.
Because alternative models wouldn’t have worked
The objective of the Dpcm on November 6 was to flatten the curve of the second wave. Were there even gentler alternatives? Someone suggested the Swedish model, but we have seen that this is not feasible in Italy, with a larger population and consequently fewer places in intensive care. Also, the Swedish charts don’t seem to show any virtuosity.
Another model is the one proposed by the signatories of the Great Barrington Declaration, on which a later study of The lancet raised many doubts: they wanted to isolate the elderly population, leaving the rest to become naturally immunized; But community immunity cannot be achieved naturally; nor did the Great Barrington signatories explain how it would be possible to keep all the most vulnerable subjects perfectly protected.
Read also:
[ad_2]
