
[ad_1]
While the evidence of the blockade is evaporating, so is the support for that same strategy that is rapidly declining. We can no longer keep silent and comply, say the writers. (Photo: Unsplash / Giacomo Carra)
Covid-19 could well be remembered as the “Panic Pandemic”: decisions have already been made, even more important decisions have yet to be made. We present a case for your consideration. We argue that suppression / blocking is not a viable strategy for this country or any other country, and never has been.
By its very nature, our argument requires a dispassionate, data-centric rather than people-centered view. There is critical data in the data that is not taken into account in the people-centered vision that currently governs politics. We are careful to postulate the blocking response hypothesis, but we deliberately avoid speculation about other elements.
NEAR
It is indisputable that we were faced with “unknown unknowns” at the beginning of this pandemic. That position has changed; there is now enough data to require a rethinking of policies. We can draw certain conclusions and postulate certain results from “known knowledge,” while requesting that as more data is collected, policy reviews should be ongoing. At the beginning of this pandemic, various models were used to formulate policies. These models (Imperial College, Oxford, IHME, SACEMA, etc.) have been shown to be demonstrably wrong. The minutiae of how they were so wrong are well recorded and do not guarantee repetition. What we do know for sure is that Covid-19 is not as fatal as initially predicted, nor has R0 reached the assumed levels.
The spread of Covid-19 has been faster in some countries, but where that is true, we also see that the infection rate reaches a tipping point and then moves towards a decreasing curve. It does not continue to extrapolate (R0 increases for a time and then begins to decrease).
How these initial models have been used to drive the blocking policy will certainly be recorded in the annals. It seems almost redundant, but completely necessary, to point out that since the 1950s, more than 300 communicable diseases have arisen or resurfaced in populations that have never been exposed to them. These include such scary examples as Lassa fever, Marburg fever, Ebola, HIV / AIDS, SARS, Zika, MERS, and swine flu. In none of these outbreaks was the world economy closed. However, we can remember the fear and fear associated with each of these events. Also, we still don’t have vaccines, despite decades of research, for some.
It is difficult to understand how the current event has caused the global suppression / blockade.
Let’s not rule out the viral diseases we are with and have been prepared to live with. The government has not considered and is not considering draconian measures for viral hepatitis, HIV / AIDS, or the flu.
However, viral hepatitis caused 1.34 million deaths worldwide in 2015, and the death rate from hepatitis has increased. Approximately 325 million people, or 4.4% of the world population, have viral hepatitis. And 1.75 million new hepatitis C infections only occur each year. At the end of 2018, approximately 37.9 million people worldwide were living with HIV. In the same year, 770,000 people died from HIV-related causes and 1.7 million people were newly infected. Worldwide, the flu causes between three and five million cases of serious illness and between 290,000 and 650,000 deaths each year, despite the fact that there is a flu vaccine.
As sure as politicians repeat the mantra “We will be guided by science,” they will also shift all the blame for faulty decision-making on to science after the pandemic. Science will be identified as the vector for economic destruction and not as the ally to face the pandemic. In some critical respects, science has a case to answer. Every day we delight in how the suppression / blocking has managed to “flatten the curve.” But the evidence to support this claim is getting thinner. Let’s not get bogged down in speculation-based comparisons and (currently) comparisons between countries with no response.
These are the facts as they are. While these charts are dense, we share them to represent key metrics.
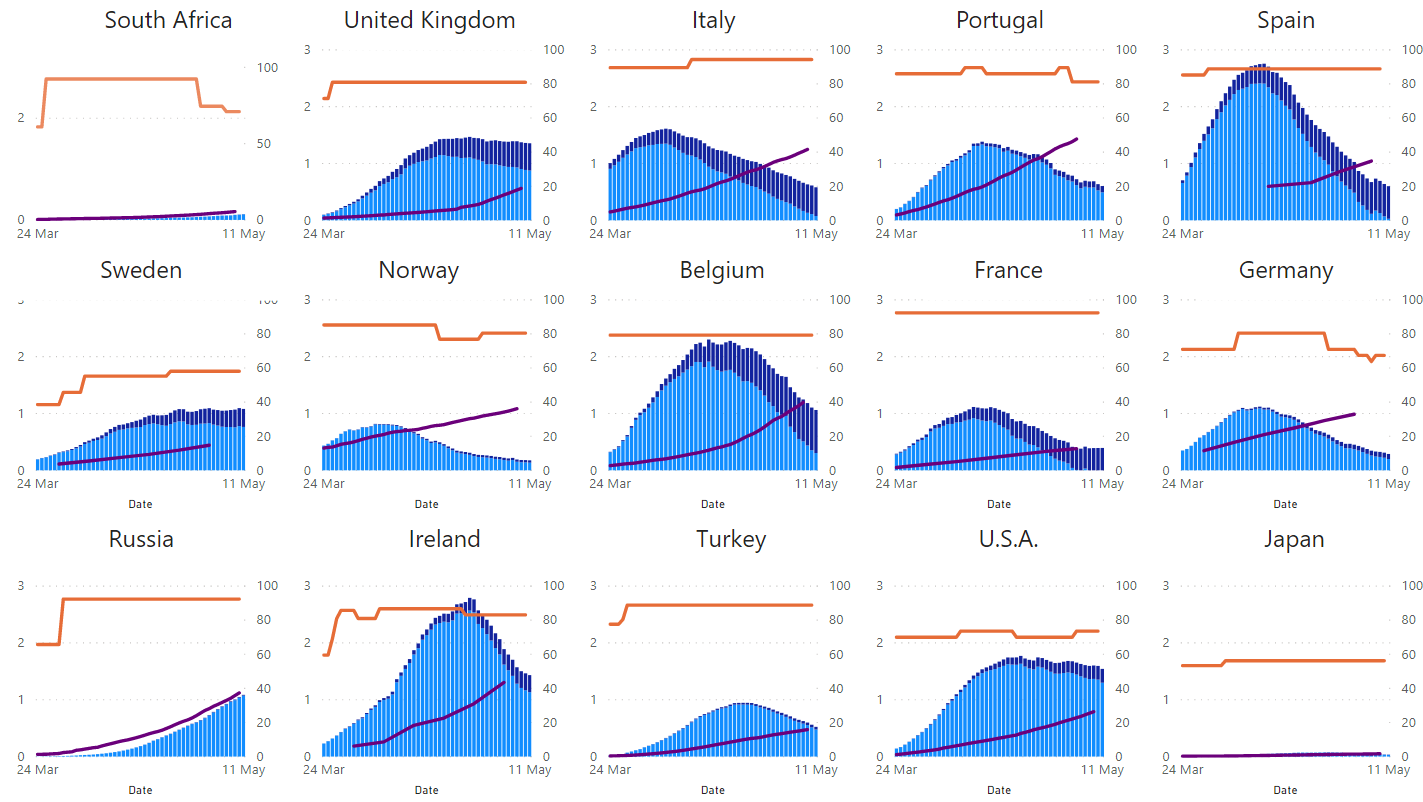
Hopefully this dispels some current myths, offered without particular order and without speculation:
- Covid-19 has been rolled out at different rates and has been established at different dates in different populations, regardless of the severity of the crash or the date of implementation.
- Covid-19 is not a runaway train. In each case described, we see a familiar pattern common to viral outbreaks. Without a doubt, Russia is at the beginning of its outbreak, while Spain, Portugal, Italy and Belgium have passed the first increase.
- The severity or earliness of the suppression / blocking does not have a predictable flattening of the curve. The countries with aggressive R0 turn out to be Spain, Belgium and Ireland. Sweden and Japan (with their much-criticized low-profile deployment strategies) stand out for their low R0s.
If you assume suppression / blocking has any efficacy, then EE. USA It will come out of the crash sooner than the data suggests. Viewing the United States as a country for this purpose ignores the differences in dates, population density, and other dynamics of the initial outbreaks at various locations, and is therefore deeply flawed. A cursory glance at Johns Hopkins Board will attest to this.
Or see the confirmed cases by subregion (R0):
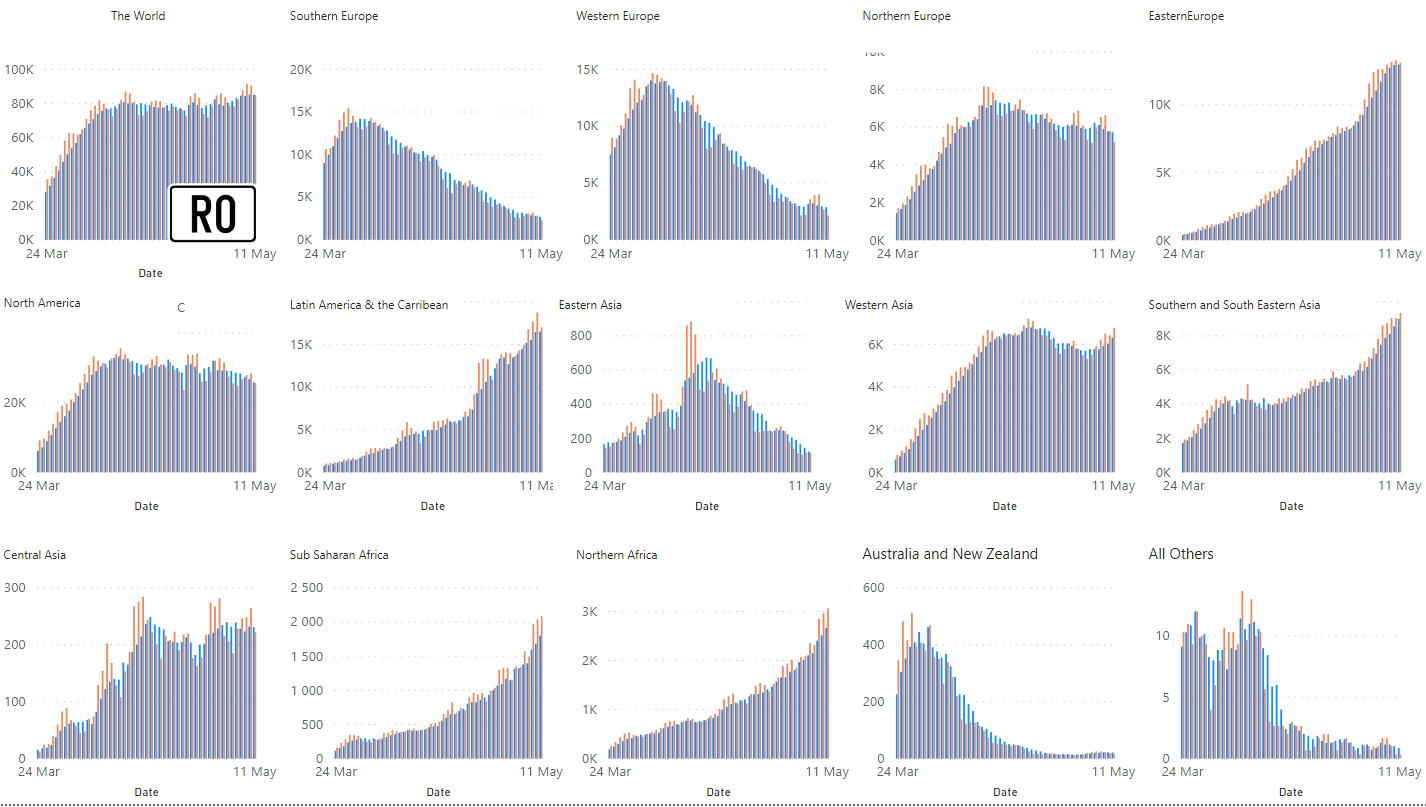
Blue Column – 7 day average
The Y axis is scaled based on data from the region.
The problem with absorbing the compelling message these charts represent is that they are snapshots of a disease at different trajectories in the cycle. By considering 1,000 confirmed cases as Day 1 of the outbreak, we can trace the path of the curve for each country from the same relative starting position. In fact, there are some surprisingly similar trajectories for countries: what is
The bottom line is that the path of infection is determined by population size (an indicator of geographic size or population density).
By this resource, all possible variables are removed from the equation (climate, health capacity, strict restriction, to infinity). The results are nothing less than surprising:
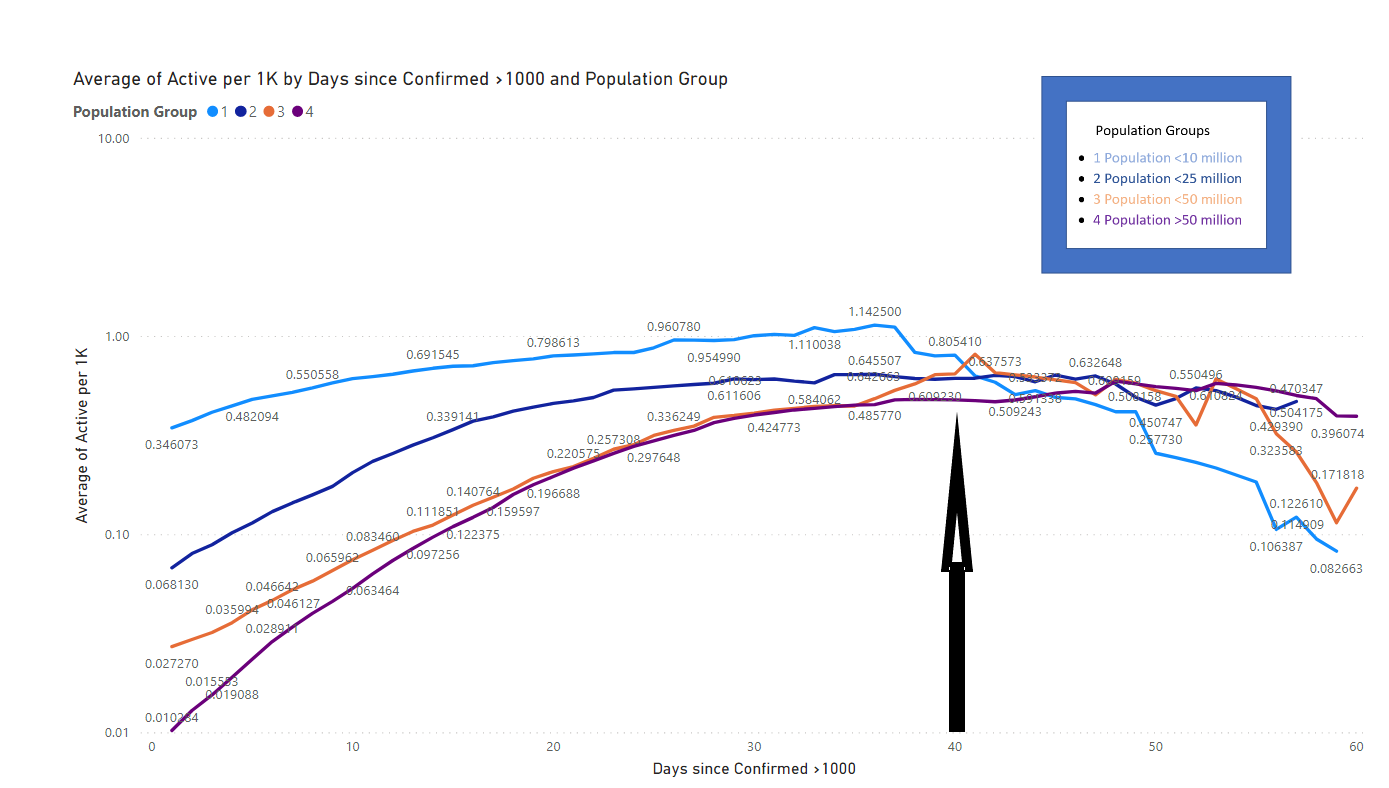
While there is wide divergence in active cases on day 1, the disease spreads through the population on a trajectory that culminates in a very narrow band of active cases on day 40. Be careful to look to the right of this date as the sample size begins to lose weight But it cannot go unnoticed that the active rate is in decline.
Then there is the question of demographics. Medical science received a “closed population” experiment (under unfortunate circumstances) as early as February for the Diamond Princess cruiser and in late March for the USS Theodore Roosevelt. We chose these two examples because of the obvious disparity in the demographics of their age.
The princess, who has an average passenger age of 68, and the naval ship presumably has a young and healthy population.
The test ratios in both cases were orders of magnitude higher than the figures recorded for the countries for obvious reasons. Several things stand out: the infection rate was no different, 18.9% and 15.1%. Most tellingly, although the population size was similar, from 3,711 to 4,500, the death rate was 0.32% (12 deaths) compared to 0.02% (one death) on naval vessels and 20% hospitalization rates for Princess Diamond, compared to 1.03% for Roosevelt.
Initially it was reported that 80% of patients on the Diamond Princess showed little or no signs of the disease. This was an early and forceful indication that the elderly had a significantly increased risk of contracting the virus. Furthermore, even in the vulnerable elderly age group, severe illness occurs in a minority.
Subsequently there have been many confirmations, not limited to:
Italy as of May 4, 2020. Of the total deaths, 25,635 (95.3%) were 60 years of age or older.
United States as of May 1, 2020. Of the total deaths, 34,343 (92.05%) were 55 years of age or older.
It is obvious that people with the highest risk of Covid-19 are not in the population group that drives the economy, and even less in the learning group. Even with the limited data available in South Africa, older people with comorbidities are clearly the most affected in our population.
Confronting economic and health costs with each other, as if there were a tradeoff between the two, is false at best and negligent in history at worst.
The simultaneous destruction of both the demand and the supply of the economy in any period is a high risk bet; over a long period of time the risk is extrapolated (this is critical, not linear).
Although we do not claim to have an economic background, there may be little or no doubt that the decision to close (for 21 days) and the subsequent hesitation to lift the blockade will have disastrous effects in our country.
The reasoning currently offered by the government in defense of its position, and as a justification for the excess of its powers, does not withstand even the most lax scrutiny. According to the government’s own admission, we have been thrown into an abyss.
SARS predicted a deficit of R285 billion in tax revenue. The Treasury has stated that in the best case scenario (where the economy recovers, an extraordinary principle in an economy strangled by the government) we will have lost three million jobs, seven million in the worst case scenario (the one we currently choose) be in). In perspective, the 2009 financial crisis “alone” cost less than a million jobs, and yet the consequences were dire.
The economy must reopen, not in the staggered way that is currently exposed. It should reopen as quickly as possible. Decision making must be restored to the system, not the government. Government interventions of this magnitude have a checkered history (at best). Let society set the new standard. Let companies (directors and employees) solve the challenges of physical distance, hygiene, testing, etc. Now, more than ever, the feeling of need for cooperation between science, industry, government, population and medicine is at an unprecedented peak: let us take advantage of that feeling to obtain positive results.
A vaccine may or may not be developed in the next year. Seroprevalence tests will give us a better understanding of the characteristics of this particular virus with regard to infectivity and immunity. At the end of the day, Covid-19 will not go away. We will have many more infections and more deaths. We will probably face an increase in winter (as with many respiratory viral infections).
While the loss of a single life from Covid-19 is tragic, the active increase in concomitant loss of life and impoverishment of millions is preventable. There can be little doubt, if any, that the loss of life caused by the blockage will far outweigh the loss of life from the virus. This has been the case elsewhere historically; For example, the measles outbreak (a direct consequence of an unbalanced health system focused predominantly on a single disease), following the Ebola outbreak in West Africa, claimed twice as many lives attributed to Ebola. Shaking the South African unemployment rate from 27% to over 50%, death has been great.
What we need now is decisive and reasoned action. It may not be popular in the short term, but this is not the time for political scoring. Leadership is not just about making the right decisions; it is making civil society make those decisions. While the evidence of the blockade is evaporating, so is the support for that same strategy that is rapidly declining. We can no longer be silent and obedient. We need bold and decisive leadership; we need to demonstrate flexibility in light of the emerging evidence. We need to continue disinfecting. We need to protect the elderly and people with comorbidity, but not at any cost. We need to continue to improve testing and health service preparedness. We need to abandon the strategies that do more harm than good, and we need to rescue our economy and the 2020 academic calendar for all levels of education, recognizing that there will be a price to pay. We need to act now.
The current position of the South African government on repression / blockade should be clearly focused with this graph (expanded from above with the Y axis in proportion). The blockade has not “flattened the curve”, despite being in place for six weeks
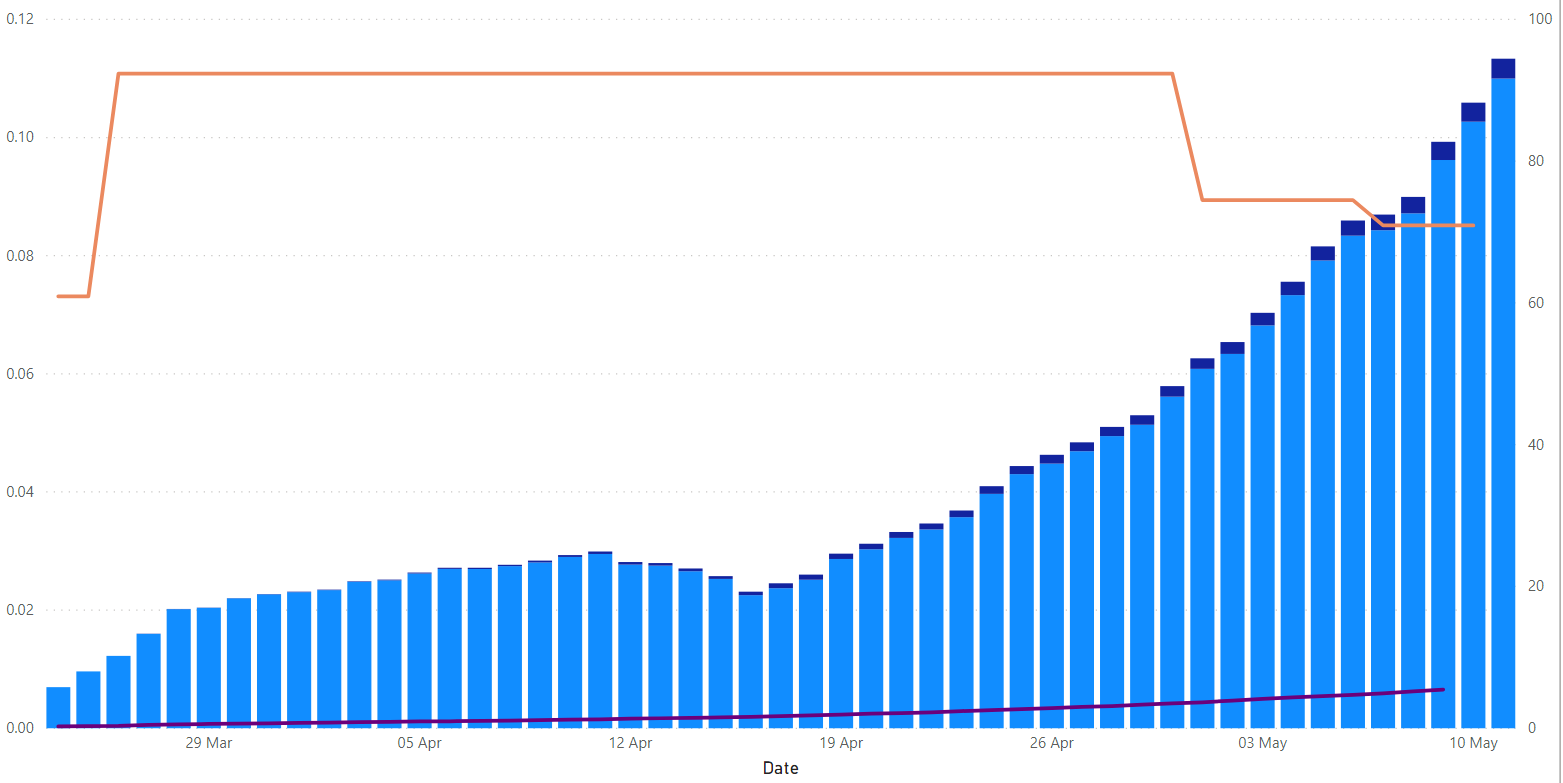
The infection rate has increased substantially and in fact accelerated after deletion / blocking. And consider that the South African tests only increased significantly weeks after the blockade was decided as a strategy.
Is the chart above enough to justify the current blockade, or is any chart from any country in the world enough to satisfy our government’s position? We say an emphatic no.
We invite you to test our hypotheses against any country in the world. The board is available at coronavirus.africa.com. DM
Professor John Gear was previously Head of Public Health at the University of the Witwatersrand and Founding Director of the Rural Facility at the University of the Witwatersrand and, currently in retirement, Medical Director of the Tshemba Foundation who recruits volunteer health professionals for rural north from Mpumalanga.
Ian McGorian, “Datanaut” provided the mathematical and statistical expertise underpinning the article.
![]()
Comments: share your knowledge and experience
Please note it must be a Maverick Insider to comment. Register here or if you are already an Insider.
